



 Facio Scapulo Humeral (FSH, FSHD) Muscular Dystrophy Genetic Test
Facio Scapulo Humeral (FSH, FSHD) Muscular Dystrophy Genetic Test
What is Facioscapulohumeral Muscular Dystrophy?
Facioscapulohumeral muscular dystrophy (FSHD) is a genetic muscle disorder that is one of the most affected groups of our face, shoulder blades and upper arms.
Facio is a Latin medical term for faces; The anatomical term and Latin word for shoulder blade is scapula. The humerus is the anatomical term for the bone in the upper arm from the shoulder to the elbow. Muscular is the Latin word for muscle.
Dystrophy; It refers to progressive muscle degeneration, with increasing weakening and atrophy (mass loss) of the muscle. In FSHD, weakening severely affects our face first, then our shoulders and upper arms, but the disease often causes weakness in other muscles.
“Istanbul Laboratory has added the FSHD Test to the working list and is being studied.”
What are the Symptoms of FSHD?
FSHD usually begins before age 20, with weakening and atrophy (loss) of muscles around the eyes and in the mouth, shoulders, upper arms, and lower legs. Later, the weakness may spread to the abdominal muscles and sometimes to the hip muscles.
Some doctors divide FSHD into adult-onset and childhood-onset types. Adult-onset cases (including FSHD in adolescence) are much more common.
In both types of FSHD, facial weakness can begin in childhood. Sometimes, other FSHD symptoms appear in early childhood. Childhood-onset FSHD usually has a more pronounced course in terms of muscle weakness and can sometimes lead to hearing and vision loss.
Preliminary symptoms suggest that the infantile onset form is associated with a larger piece of DNA than missing. The age of onset, progression, and severity of FSHD vary widely.
Usually symptoms develop during the teenage years and although most people notice some problems by the age of 20, weakness of some muscles can begin in infancy and begin as early as the 50s. In some people, the disease may be mild, with no symptoms being noticed. In these cases, the disease can only be diagnosed after another witness, with the more affected family member coming to medical care.
People with FSHD often don’t go to the doctor until their shoulder or leg muscles are involved and have trouble reaching their head or stepping stairs. Many people may recall experiencing symptoms in childhood when questioned, covered shoulder blades, or difficulty throwing the ball. Often times, people say they’ve never churned or blown whales or stuck a drink in a straw, but they may not have associated these issues with muscular dystrophy.
FSHD does not cause learning disabilities or other cognitive impairments; it also does not affect sensation, bladder and bowel control ability, or sexual functions. In most FSHD patients, the disease progresses very slowly. It can take up to 30 years for the disease to become severely ineffective, and it doesn’t happen to everyone. Estimates are that about 20 percent of people with FSHD use a wheelchair at least some times. For more information on corrective measures for some of these symptoms, see Medical Management.
Abdominal Muscle Weakness
Many people with FSHD have abdominal muscle weakness. These may weaken at the beginning of the disorder. As abdominal weakness progresses, lordosis develops, an exaggerated curve in the lumbar (lower) region of the spine.
Abnormalities of the Retina
Certain abnormalities in the retinal blood vessels, the “curtain” at the back of the eye through which visual images are projected, are often detected in people with FSHD. Fortunately, a small number of people will not have any vision problems due to it, but should be monitored by an ophthalmologist. For reasons that are not clear, the problem is usually more common in infantile-onset FSHD. The source of the retinal problem is not well understood in either form of the disease.
Cardiac and Respiratory Functions
Although cardiac involvement can sometimes be a factor in FSHD, it is rarely severe and is usually only discovered through specialized testing. Some experts have recently recommended monitoring of cardiac function with FSHD.
The muscles used for breathing are not affected by FSHD, as are other forms of muscular dystrophy. However, for some patients it may be advisable to test pulmonary function at intervals.
 Face Weakness
Face Weakness
Facial weakness is the first sign of FSHD. It may not be immediately noticed by people with FSHD and is often noticed by someone else.
The muscles affected are those surrounding the eyes and mouth. It’s hard to smile or stand up or have more strength in the mouth, so people with the disease have trouble with balloons, straws, and whistles.
Weakness in the eye muscles can prevent the eyes from closing completely during the night. As the disease progresses, the eyes sometimes dry overnight, which can injure them. Waking up in the morning with gritty, burned, or dry eyes can be a sign of incomplete eye closure. It may be necessary to wear an eye shield or correct the eyes during sleep. Facial weakness can make it difficult to make a gesture or smile.
Weakness in the Hip
In some people, weakness of the hip muscles surrounding the pelvis (arch area) also occurs. This doesn’t happen to everyone. Weakness of the hips appears to occur on its own in middle adulthood. Hip infertility creates problems with rising from a chair or stair talks, and a wheelchair may be needed, especially for long distances. Upper leg muscles are also sometimes affected. Abdominal girdle weakness can result in a strenuous gait and contributes to lordosis (inward tilt) often seen in FSHD.
Hip weakness in children with FSHD may be the first thing parents notice because it causes problems with walking and running.
Joint and Back Abnormalities
As the muscle weakness prolongs, it can cause the skin to freeze in a position called contracture (shortening of the muscle). If contractures occur in FSHD, they will likely be in the ankle joints.
The spinal column actually consists of many joints between the vertebrae. The spine is designed to be flexible like a flexible toy, so the column pulls out of alignment as the muscles surrounding the spine weaken.
Misalignment often takes the form of lordosis; the spine here is excessively curved and the abdomen leaks. But it can also take the form of scoliosis, where the spine curves like an S. Scoliosis (curvature of the spine) sometimes seen in FSHD is not serious.
Lower Leg Muscle Weakness
As FSHD progresses, the front and side muscles in the lower legs often weaken. While walking, the muscles that allow us to lift the front of the foot weaken and therefore prevent us from walking normally.
As these muscles weaken, the foot lags behind after pressing during walking, sometimes switching to walking. This condition is called foot drop.
The doctor may say, “Walk in heels, like a penguin,” to test the strength of these foot lift muscles.
People will say “like I caught my foot while walking” or “like I fell on my own feet”. Trouble walking on stairs and uneven surfaces. Not everyone with FSHD will experience this lower leg problem.
Mild Hearing Loss
Hearing loss sometimes occurs in FSHD, but is usually mild and often affects high-pitched sound perception. It is usually not noticed until carefully tested (Odio Test). In adult-onset FSHD patients, some experts have investigated whether hearing loss is more common in adults overall. The cause of hearing loss is not clear when it occurs.
When FSHD begins in childhood, the higher range of hearing loss may be more profound than adult-onset FSHD. The reason for this is not yet understood.
Pain and Infection
Inflammation of the muscles – attacks of certain immune system cells or seen in some muscular dystrophies. It may be common in some people with FSHD. For this reason, FSHD is sometimes misdiagnosed as another type of muscle disease, polymyositis, a non-genetic disorder in which the immune system attacks the muscles. An important difference is that polymyositis can be treated with prednisone, a cortisone drug that suppresses inflammation, but prednisone does not affect the course of FSHD. The many side effects of cortisones make them unusable just to relieve discomfort.
The pain in FSHD can also come from the way weakened muscles push bone structures like the spine and shoulder blades out of alignment.
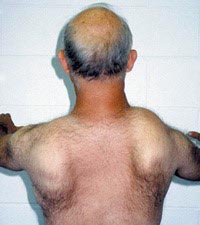
 Weakness of the Shoulder
Weakness of the Shoulder
Muscles that are not normally visible from the front can be seen in FSHD because of weakness in the shoulders and back. Most FSHD patients notice weak muscles in the shoulder blade area (scapula) as the first sign that something is wrong. The shoulder blades are normally fairly fixed in their position. They act as the fulcrum allowing the arm muscles to take leverage to lift things, including their own weight.
In FSHD, the muscles holding the shoulder blades in place weaken, allowing these bones to move excessively. Because the protruding bone resembles a wing, the shoulder bridge bones rise toward the neck as it moves. This is also called “paddle wing”. The leverage is at least partially lost. Weakness is not usually the same on both sides of the body. This person also shows a typical unsymmetrical pattern of weakness, with scapular wings and mild scoliosis.
Early on, the person with FSHD realizes that they cannot throw a ball effectively. Then it can be difficult to lift the arms over the head to do their hair or reach a high shelf or hang something. These problems are due to weakening of the muscles around the shoulder and upper arm.
Unsymmetrical Weakness
In most FSHD patients, the weakness is at least slightly different between the left and right sides of the body. In some people with FSHD, the difference between these two sides can be quite striking. The reason for the lack of symmetry that is not seen in most types of muscular dystrophy is not clear.
 What Causes FSHD?
What Causes FSHD?
FSHD can be passed on from the father or mother, or it can happen without a family history. It is often associated with a genetic defect (mutation) on chromosome 4 that causes a shorter-than-normal section of DNA. The segment is not part of any particular gene, but still appears to interfere with the correct processing of genetic material. A small number of individuals have a disorder similar to FSHD but without a short segment on chromosome 4. The genetic cause of their disease has not yet been determined.
Inheritance
In fascioscopeulohumeral muscular dystrophy (FSHD), a small portion of DNA on chromosome 4 that is shorter than normal is inherited from an autosomal dominant pattern; receives such a mutation from only one parent to cause this disorder. This altered piece of DNA can also arise spontaneously in a child as it develops in the womb.
FSHD can affect either males or females. In a small number of people with FSHD, a normal chromosome 4 mutation cannot be identified. In most affected people, it may be through genetic testing.
FSHD is one of many genetic disorders in which germline mosaicization is thought to occur. Germ line refers to egg or sperm cells. In this phenomenon, some sperm or egg cells in a parent carry a particular mutation.
In families with more than one child with FSHD but no previous family history, one parent has germline mosaicism and these affected children are carried with the egg or sperm cells that carry the FSHD mutation. In these cases, the parents have no symptoms and will not show this mutation if genetic testing is done.
It would be best to speak with a genetic counselor for help with understanding the specific situation of your family and planning for future children.
How Will FSHD Progress?
FSHD usually progresses very slowly and rarely affects the heart or respiratory system. Most people with FSHD Disease have a normal lifespan.
How is FSHD Research?
In 2009, genetic researchers discovered that a fragment called DUX4 is abnormally activated in cells affected by FSHD, causing the production of potentially toxic proteins. Blocking accidentally activated genes or the proteins produced from them seems to be a possible avenue for the ultimate treatment of FSHD.